วันที่ created 26 มิ.ย. 2565 10:38 วันที่ edited 8 มิ.ย. 2568 21:46 | เข้าชมแล้ว 2241 | admin3
A 70-year-old female, presented with arthralgia at both wrists and ankles for 1 mo. She complained of fatigue, dyspnea on exertion, low-grade fever, and 3-kg weight loss in the past 3 mo.
Physical examinations:
- BT 37.7 C
- No definite joint swelling, erythema, and warmth
- Liimitation of ROM of bilateral fingers, wrists, ankles
- Decreased breath sounds at Lt lung field
Questions
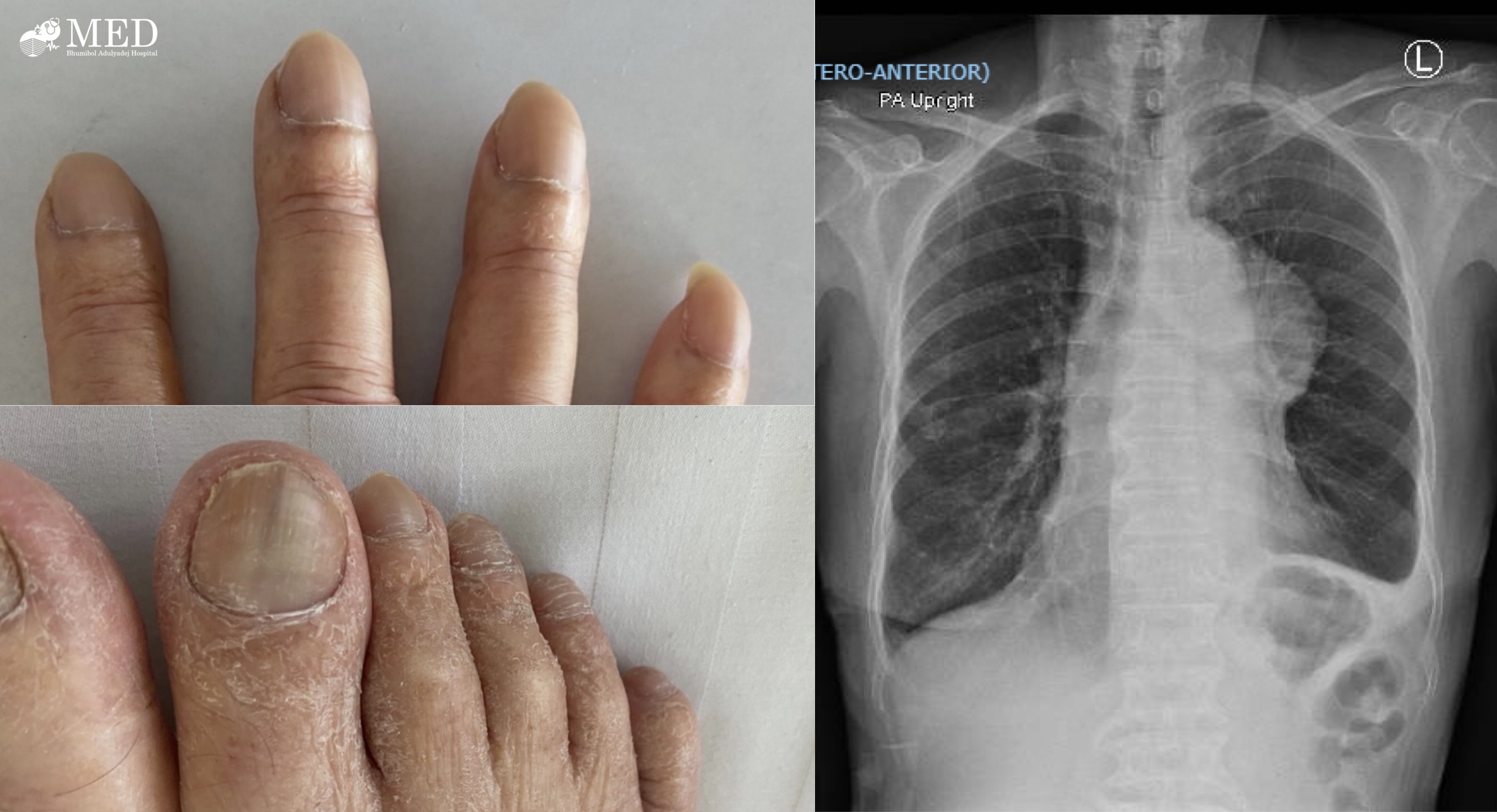
1. Please describe the other abnormal clinical findings and the radiographic findings
2. What is the provisional diagnosis?
3. What is the plan for further investigations and management?
โดย นพ.จิตรณรงค์ กาฬมณี แพทย์ประจำบ้านชั้นปีที่ 3 กองอายุรกรรม รพ.ภูมิพลอดุลยเดช กรมแพทย์ทหารอากาศ
ANSWERs
1. Abnormal clinical and radiographic findings
- Clinical: clubbing of fingers of fingers (may perform Schamroth sign) and toes
- CXR: suspect mediastinal mass with Lt pleural effusion
2. Provisional diagnosis: Hypertrophic osteoarthropathy (HOA)
- Associating conditions may include
- Primary HOA (3%): often male with positive family history, pachydermoperiostosis
- Secondary HOA (97%): 90% due to intrathoracic infections or malignancy
- Lung cancer (Adeno CA > Small cell CA)
- Metastatic lung cancer
- Pleural mesothelioma
- Esophageal carcinoma
- Other malignancies: Hodgkin lymphoma, HCC, renal cell CA, rhabdomyosarcoma
- Pulmonary infections (e.g.TB)
- Cirrhosis, infective endocarditis, primary sclerosing cholangitis
- Childhood HOA: cystic fibrosis, right-to-left cardiac shunt
- Pathogenesis
- VEGF, PDGF from CA lung to distal bone
- Prostaglandin E2
- Excessive collagen deposition, endothelial hyperplasia, edema, new bone formation
3. Plan for investigations and management
- Investigations:
- Work up etiology of mediastinal mass, other associated conditions that could cause HOA
- Film long bones:
- Laminated or onion-skin periosteal reaction (periostitis) at diaphysis with spared epiphysis, with cortical thickening, more prominent at lower > upper extremities, no joint space narrowing, no erosion
- Acroosteolysis in long-standing HOA or cyanotic heart disease
- Bone scintigraphy: linear subperiosteal increased uptake at shaft of long bones
- Management
- Treat primary cause of HOA (malignant thymoma in this case)
- Treat pain by inhibiting further periostitis: NSAIDs, anti-VEGF (eg.octreotide, bisphosphonate)


References: Kelley's Textbook of Rheumatology 11th ed, EULAR Textbook of Rheumatology 3rd ed
#rheumato #CXR #skin #HOA
เรียบเรียงโดย นพ.สุวิชช์ บุญญาจรัสกุล แพทย์ประจำบ้านชั้นปีที่ 3 และ นพ.กฤตณัฐ เตชพาหพงษ์ และ พญ.วิรัลพัชร มาศมหิศักดิ์ แพทย์ประจำบ้านชั้นปีที่ 2 กองอายุรกรรม รพ.ภูมิพลอดุลยเดช พอ.