วันที่ created 26 ก.ย. 2565 23:15 วันที่ edited 8 มิ.ย. 2568 22:38 | เข้าชมแล้ว 6136 |
A 51-year-old female, unknown underlying disease, presented with dyspnea on exertion for two weeks. Chest radiography revealed bilateral pleural effusion.
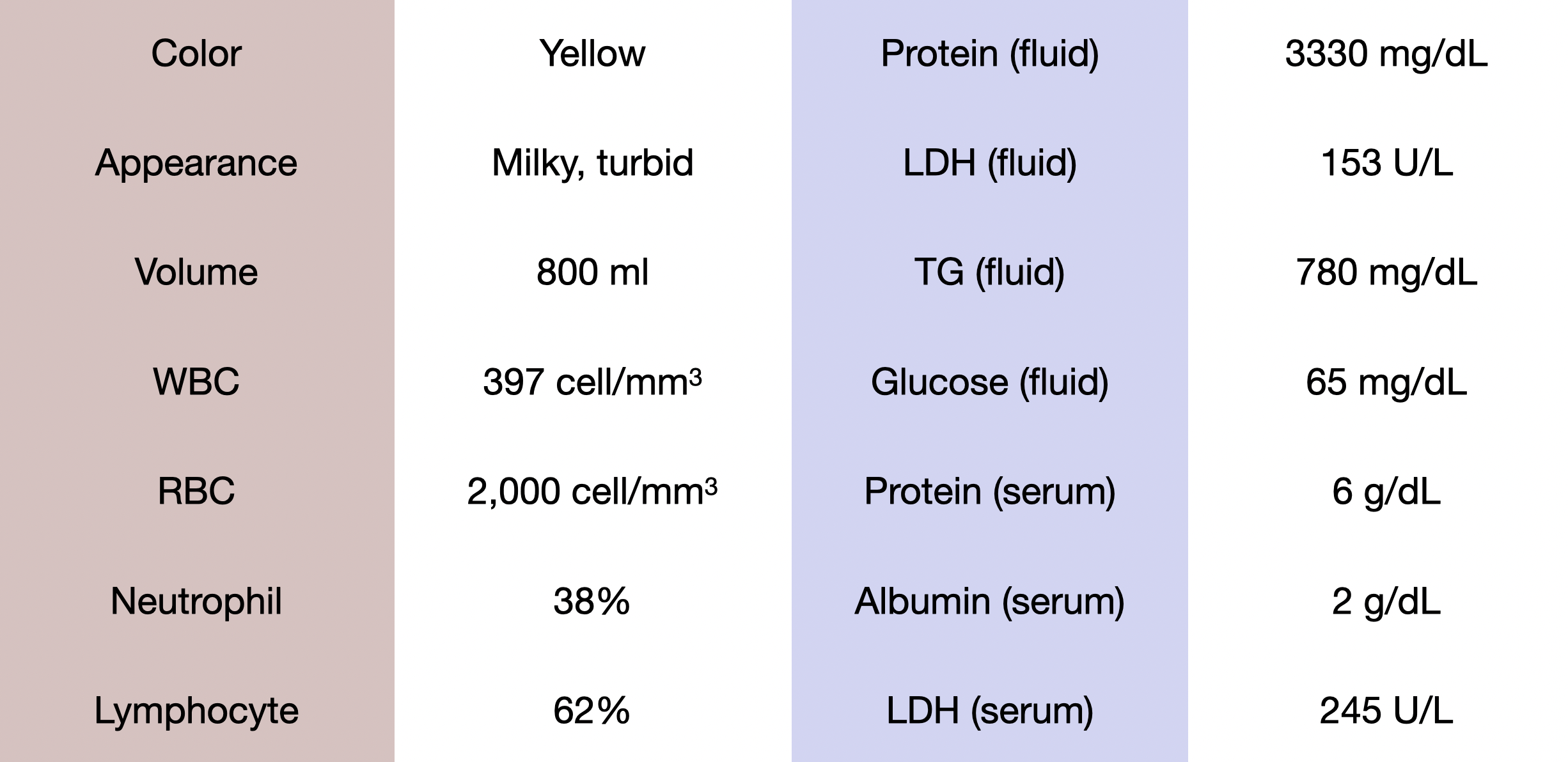
Thoracocentesis was done on the right side and the results are shown below.
Questions:
1.Please interpret the pleural fluid results
2.Please give differential diagnosis
3.What is the proper next step investigation and management?
โดย น.ท.หญิง อินทิรา อุไรเลิศ หัวหน้าหน่วยโรคข้อและรูมาติสซั่ม และภูมิแพ้ กองอายุรกรรม รพ.ภูมิพลอดุลยเดช กรมแพทย์ทหารอากาศ
ANSWERs
1. Interpretation of the pleural fluid results
- จากลักษณะสีของ pleural fluid ที่มีลักษณะเป็น turbid สามารถบ่งบอกถึง ความเป็น exudative profile ได้เบื้องต้น
- หากนํามาเปรียบเทียบ Light's criteria จะพบว่าเข้าได้กับ criteria ทั้ง 3 ข้อ ได้แก่
- 1. PF/serum Protein (3.33/6 = 0.55) > 0.5
- 2. PF/serum LDH (153/245 = 0.62) > 0.6
- 3. PF LDH > 2/3 upper limit of normal of serum LDH (153 > 142) (reference range upper limit of LDH= 214)
- ลักษณะ milky pleural fluid สามารถนึกถึงได้ 3 กลุ่มโรคได้แก่ chylothorax (ตรวจพบ triglyceride สูง), pseudo chylothorax (ตรวจพบ cholesterol สูง), empyema thoracis (ตรวจพบ bacteria จากการย้อม gram stain จาก pleural fluid)
- Film chest x ray ไม่พบลักษณะ loculated pleural effusion ที่อาจเป็น empyema thoracis ได้ และ differential cell count เป็น lymphocyte predominate จึงคิดถึงสาเหตุจาก chylothorax, pseudo chylothorax มากกว่า ซึ่งสามารถยืนยันด้วยการส่งตรวจ triglyceride และ cholesterol
- ปกติเกณฑ์ cut off value ของ triglyceride ใน effusion chylothorax อยู่ที่ 110 mg/dl แต่ถ้าหาก triglyceride ใน effusion มากกว่า 240 mg/dl จะมี sensitivity และ specificity >95%
- ระดับ triglyceride ใน effusion ของผู้ป่วยรายนี้อยู่ที่ 780 mg/dl ซึ่งถือว่า definite ว่าเป็น chylothorax อาจไม่ต้องส่ง cholesterol level ใน effusion ก็ได้
2. Differential diagnosis
- การ approach chylothorax สามารถ approach ได้ตาม etiology โดยแบ่งออกเป็น
- 1. Traumatic cause เกิดจากการมี injury ต่อ thoracic duct สามารถเกิดขึ้นได้จากอุบัติเหตุหรือ iatrogenic จาก intrathoracic surgery หรือ การใส่ central venous catheter ก็ได้ แต่เนื่องจากในผู้ป่วยรายนี้ไม่มีสาเหตุดังกล่าวจึงคิดถึง non traumatic cause มากกว่า
- 2. Non-Traumatic cause สามารถแบ่งได้ออกเป็น malignancy related และ non-malignancy related โดยส่วนใหญ่จะเป็นสาเหตุจาก malignancy มากกว่า
- สาเหตุจาก malignancy related พบได้ใน malignancy ที่มีการ invasion เข้าไปใน mediastinum ซึ่งสามารถ invasion หรือ compression thoracic duct ได้ สาเหตุ ได้แก่ lymphomas, CLL, lung cancer, mediastinal cancer (germ cell tumor, thymic carcinoma), metastatic cancer, Kaposi sarcoma หรือการได้รับ thoracic irradiation ก็สามารถเป็นสาเหตุได้
- สาเหตุจาก non-malignancy related สามารถแบ่งออกได้เป็น 1. Benign tumors เช่น thymoma, goiter 2. Infections เช่น tuberculosis, histoplasmosis, filariasis 3. Autoimmune diseases เช่น SLE, Behçet's syndrome, sarcoidosis, IgG4-related disease 4. Congenital and genetic diseases เช่น lymphangioleiomyomatosis (LAM), Noonan syndrome, Turner syndrome
- ในผู้ป่วยรายนี้ สาเหตุที่ควรคิดถึงมากที่สุดอาจเป็น 1. Malignancy cause เนื่องจาก age group 2. Infection ซึ่งต้อง rule out โดยเฉพาะ tuberculosis เนื่องจากอยู่ใน endemic area 3. Autoimmune diseases เนื่องจากผู้ป่วยเป็นเพศหญิงซึ่งมีโอกาสเกิด autoimmune diseasesได้อยู่แล้ว แต่อาจจะต้อง exclude malignancy และ infection ออกไปให้ได้ก่อน
3. Next step investigation and management
- การ investigations เพื่อหา etiology ของ chylothorax ในผู้ป่วยรายนี้ ได้แก่
- 1. CT chest with whole abdomen: เพื่อหาว่ามี mediastinal mass ซ่อนอยู่หรือไม่ หากพบว่ามี ascites ในช่องท้องร่วมด้วยอาจเป็น chylous ascites ในช่องท้อง leak เข้ามาใน pleural cavity ได้เช่นกัน
- 2. หา Infection: work up TB เช่น sputum AFB, PCR for TB หรือ gene expert for TB of pleural fluid, check immune status ผู้ป่วย เช่น anti-HIV, check cbc ดู blood eosinophil
- 3. หา Autoimmune diseases: หากประวัติและ clinical สามารถเข้าได้กับ autoimmune disease อาจส่ง ANA profile, anti-dsDNA, anti-Sm เพื่อ screening หา SLE
- การ management chylothorax ในผู้ป่วยรายนี้แบ่งออกได้เป็น
- 1. Pleural drainage to control symptoms เนื่องจากผู้ป่วยรายนี้มี bilateral pleural effusion มี dyspnea on exertion การ drainage สามารถลด symptom ของผู้ป่วยได้ สามารถทํา intermittent thoracocentesis หรือ chest tube drainage ก็ได้ แต่ต้องเฝ้าระวังในผู้ป่วยที่ on chest tube เป็นเวลานานอาจทําให้ผู้ป่วยเกิด immunosuppression ได้จากการสูญเสีย lymphocytes และ immunoglobulins และ malnutrition จากการสูญเสียไปพร้อมกับ effusion
- 2. Dietary modification: แนะนําให้ผู้ป่วยรับประทานอาหารที่เป็น medium chain fatty acid เนื่องจากจะสามารถดูดซึมเข้า blood circulation เข้าไปทาง portal vein ได้โดยตรง โดยลดการดูดซึมผ่านทาง lymphatic duct จึงลด chyle producing ในผู้ป่วยที่มี high-volume chyle leaks คือ มี chylothorax วันละมากกว่า 1 L พิจารณาให้เป็น total parenteral nutrition (TPN)
- 3. Treatment of the underlying condition: ในกรณีที่ failed medication treatment อาจพิจารณา surgery หรือ intervention เช่น thoracic duct ligation หรือ thoracic duct embolization ต่อไป
#chest #chylothorax
เรียบเรียงโดย นายแพทย์สรสักก์ จันทร แพทย์ประจำบ้านชั้นปีที่ 2 กองอายุรกรรม โรงพยาบาลภูมิพลอดุลยเดช กรมแพทย์ทหารอากาศ
Reference: Agrawal A, Chaddha U, Kaul V, Desai A, Gillaspie E, Maldonado F. Multidisciplinary Management of Chylothorax. Chest. 2022 Jun 20:S0012-3692(22)01101-1.
