Case a 68-year-old Thai female, with the underlying diseases of HT and DLP presented with progressive dyspnea for 1 month.
One month PTA, she developed dyspnea on exertion, functional class change form I -> II (NY class), dyspnea while in supine position, with night cough, with no fever, no weight gain or weight loss, no edema.
Physical examination:
Investigations:
Questions:
1. Please describe plain film findings and give differential diagnosis
2. Please tell further history taking, physical examination, and investigations for diagnosis
3. Please give proper management
โดย แพทย์หญิง วิรัลพัชร มาศมหิศักดิ์ แพทย์ประจำบ้านชั้นปีที่ 2 กองอายุรกรรม รพ.ภูมิพลอดุลยเดช กรมแพทย์ทหารอากาศ
ANSWERs
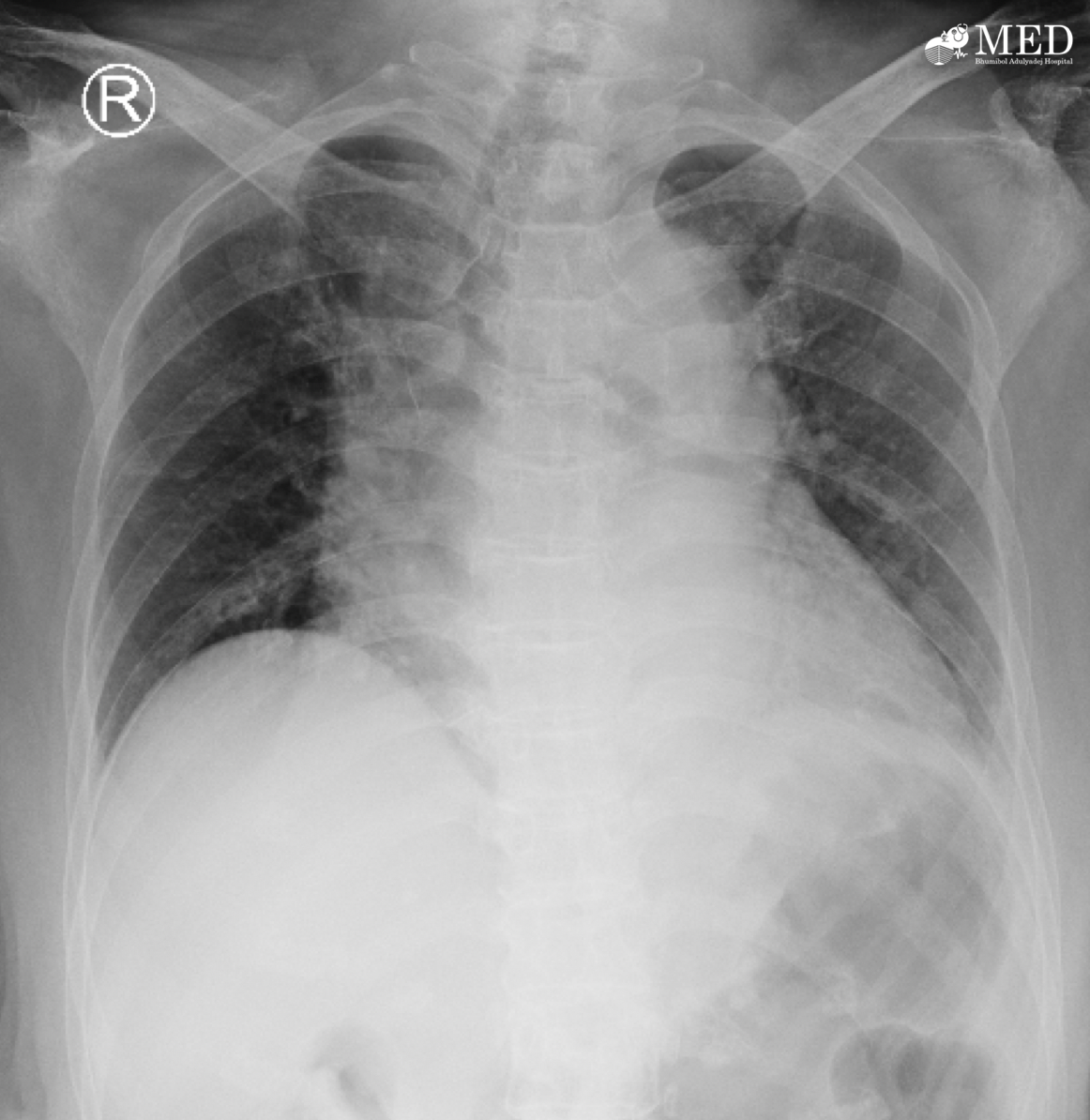
1. Plain film findings and differential diagnosis
* CXR upright position
* Exposure: adequate exposure
* Inspiration: hypoaerated
* Rotation: none
* Parenchyma: can’t evaluate due to hypo-aerated lungs
* Soft tissue: normal
* Bony: normal
* Gastric gas: normal
* Cardiac: can’t evaluate due to hypo-aeration lungs
* Diaphragm: no blunt costophrenic angle, below diaphragm normal
Differential diagnosis form small lung volume CXR
- Neuromuscular disorder: especially bilateral phrenic nerve paralysis due to hypo-aerated lungs, myasthenia gravis, Guillain-Barre syndrome
- Expiratory film
- Bilateral subpleural effusion
- Bilateral pulmonary hypoplasia
- Chest wall deformity/obesity
- Lung volume loss: atelectasis due to compressive or resorptive atelectasis
- Hepato/splenomegaly but usually unilateral
- Difficult patient: not following command
2. Further history taking, physical examination, and investigations for diagnosis
- ประวัติทางระบบประสาท เช่น อาการปวด อ่อนแรง ชา การกลั้นปัสสาวะ/อุจจาระ ระยะเวลาที่เป็น และการดำเนินโรค
- ประวัติน้ำหนักเพิ่มขึ้น
- การผ่าตัดบริเวณทรวงอกหรือท้อง ประวัติอุบัติเหตุบริเวณอก ท้อง หรือทางระบบประสาท
- เสียงขณะหายใจเข้า และออก
- การนอนกรน
- ท้องบวมโตมากขึ้น หรือคลำได้ก้อบบริเวณท้อง
การตรวจร่างกาย ควรตรวจให้ครบทุกระบบ และตรวจพิเศษตามโรคที่คิดถึง
- Lungs: sugical scar, chest expansion, adventitious breath sound
- Abdomen: distension, superficial vein, bowel sound, liver span and splenic dullness
- PR for evaluate sphincter tone
- Neuro system: cranial nerve, tremor, motor power, sensory, reflex
Investigation
- Inspiration เพื่อ rule out expiratory film
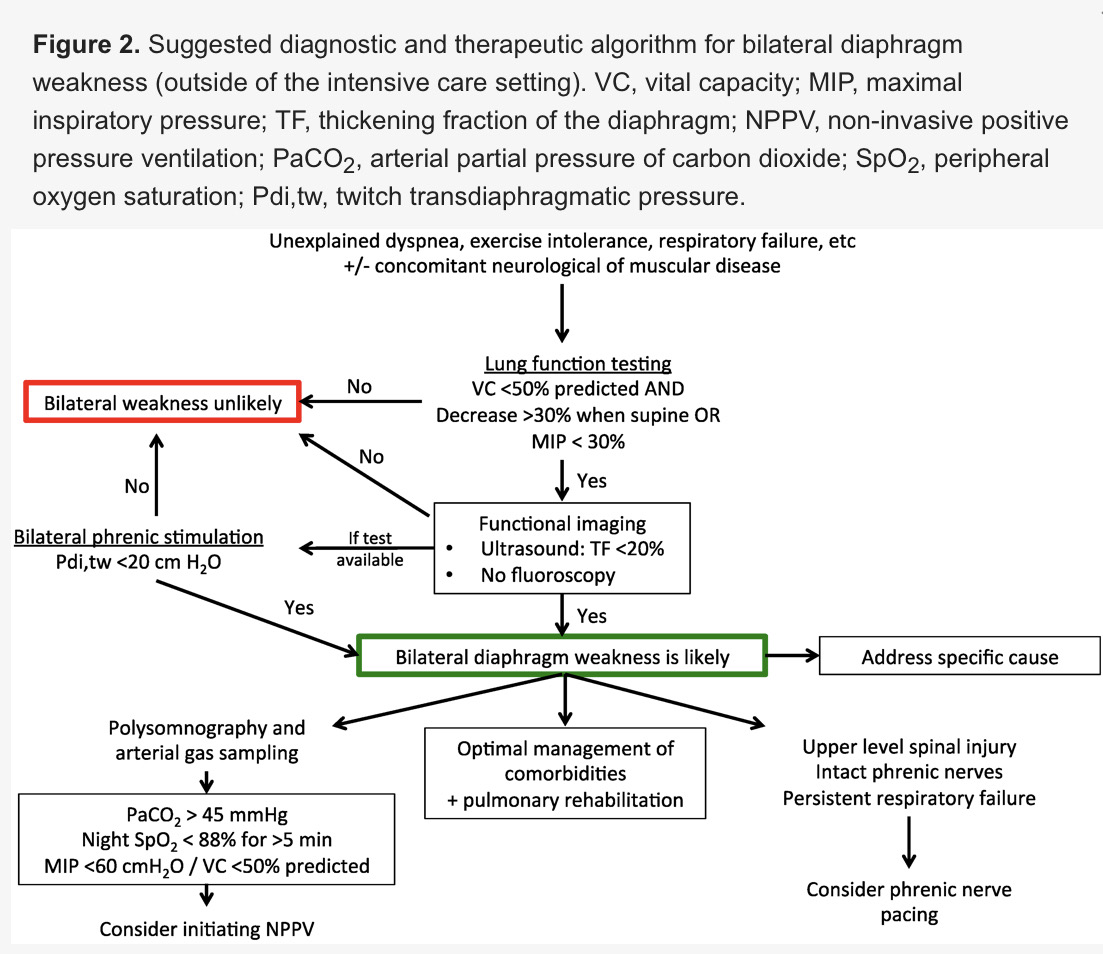
- Arterial blood gas: Neurological or muscular disease patients may reveal diurnal hypercarbia (PaCO2 > 45 mmHg) with significant nocturnal hypoventilation (SpO2<88% for >5 consecutive minutes).
- Thyroid function test
- Renal function test, electrolyte and serum albumin
- Lung function test: predicted FVC <50%
- Ultrasound: สามารถใช้เพื่อประเมินขณะหายใจได้ โดยที่ต้องให้ผู้ป่วยหายใจเอง ใช้ M mode วางที่ cranio-caudal position mid-clavicular line หากมีภาวะ diaphragm paralysis จะไม่เห็น active caudal movement ของ diaphragm และ inspiration and abnormal paradoxical movement (diaphragm ยกขึ้น) หรือมีค่า Thickening fraction of the diaphragm (TF) <20%
- Phrenic nerve stimulation: gold standard
- Investigation สำหรับโรคทาง neuromuscular disease: CT brain หรือ MRI spine สำหรับรายที่สงสัย C-spine lesion แล้วทำให้เกิด phrenic nerve dysfunction
- Fluoroscopy: สำหรับ unilateral diaphragm paralysis จะเห็น diaphragm ข้างที่ paralysis ยกขึ้นขณะหายใจเข้า
3. Proper management
ในผู้ป่วยรายนี้หลังจากการซักประวัติและตรวจร่างกาย พบว่ามีอาการอ่อนแรงแขนสองข้าง และมีอาการชา MRI spine พบว่ามี C3-4 และ C5-6 myelopathy การรักษาจึงเป็นการผ่าตัด เพื่อแก้ไข primary disease โดยอาจทำร่วมกับ phrenic nerve pacing และ rehabilitation การตรวจพบว่ามี small lung volume CXR อาจจะเป็นผลมาจากโรคอื่น ดังนั้นการรักษาจะเป็นการรักษา primary disease
Plan of investigation and management as the diagram below
เรียบเรียงโดย แพทย์หญิง วิรัลพัชร มาศมหิศักดิ์ แพทย์ประจำบ้านชั้นปีที่ 2 กองอายุรกรรม รพ.ภูมิพลอดุลยเดช กรมแพทย์ทหารอากาศ
#chest #CXR
References:
วิริสสร วงศ์ศรีชนาลัย, อดิศร วงษา, Pocket Chest Radiography; โครงการตำราอายุรศาสตร์ โรงพยาบาลพระมงกุฏเกล้า: กรุงเทพ, 2561
Lloyd, T., Tang, YM., Benson, M. et al. Diaphragmatic paralysis: the use of M mode ultrasound for diagnosis in adults. Spinal Cord 44 (2006): 505–508
DiNino E, Gartman EJ, Sethi JM, McCool FD. Diaphragm ultrasound as a predictor of successful extubation from mechanical ventilation. (2014) Thorax. 69 (5): 423-7
Dubé B-P, Dres M. Diaphragm Dysfunction: Diagnostic Approaches and Management Strategies. Journal of Clinical Medicine [Internet] 2016;5(12):113